H.5.1 Explain the events of the cardiac cycle, including atrial and ventricular systole and diastole, and heart sounds
The cardiac cycle describes the series of events that take place in the heart over the duration of one heart beat
- It is comprised of a period of contraction (systole) and relaxation (diastole)
Systole
- Blood returning to the heart will freely flow from the atria to the ventricles as the AV valves kept open by the pressure in the atria
- The sinoatrial node (pacemaker) receives signals to fire when the ventricles are almost full (~70%)
- The contraction of the atria (atrial systole) causes blood to fill the ventricles to the maximum
- The signal from the SA node is transferred to the AV node and then via Purkinje fibres to cause the delayed contraction of the ventricles
- As the ventricles contract, the increase of pressure in the ventricles closes the AV valves, causing the first heart sound ('lub')
Diastole
- The increased pressure causes the semilunar valves to open and blood to flow away from the heart
- As the blood flows into the arteries, the pressure falls in the ventricles
- This causes some arterial back flow, which closes the semilunar valves and causes the second heart sound ('dub')
- When the pressure in the ventricle drops below the pressure in the atria the AV valves open and the cardiac cycle can repeat
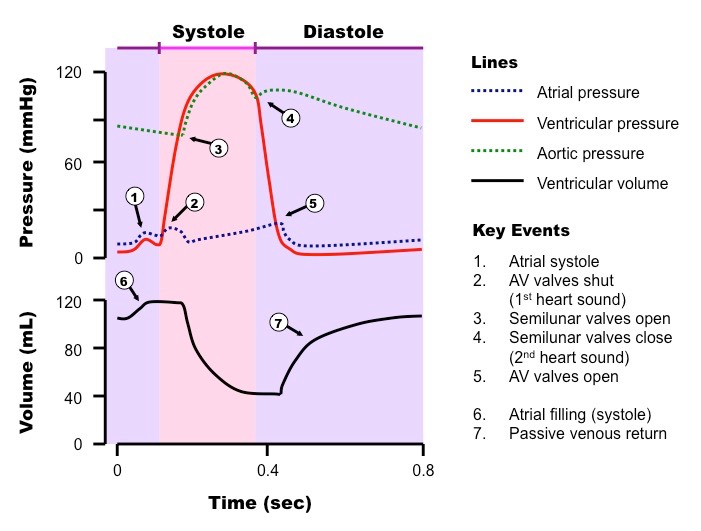
Overview of the Cardiac Cycle

H.5.2 Analyse data showing pressure and volume changes in the left atrium, left ventricle and the aorta, during the cardiac cycle
H.5.3 Outline the mechanism that controls the heartbeat, including the roles of the SA node, AV node and conducting fibres in the ventricular walls
- The contraction of the heart tissue (myocardium) is myogenic, meaning the signal for cardial contraction arises within the heart muscle itself
- Within the wall of the right atrium are a specialised plexus of nerves called the sinoatrial node (SAN)
- The sinoatrial node initiates contraction of the cardiace muscle and acts as a pacemaker, regulating normal sinus rhythm
- It stimulates atria to contract and, when excitation reaches the junction between atria and ventricles, stimulates another node (atrioventicular node)
- The atrioventricular node (AVN) sends signals via the Bundle of His to Purkinje fibres, which cause ventricular contraction
- This sequence always ensures their is a delay between atrial and ventricular contractions, resulting in maximum blood flow
- By having ventricular contractions start at the apex (bottom), it ensures blood is pushed up towards the arteries
Myogenic Control of the Heart Beat

The pacemaker is under autonomic control from the brain, specifically the medulla oblongata (brain stem)
- Sympathetic nerves speed up heart rate by releasing a neurotransmitter (noradrenaline) to increase the rate of myocardial contraction
- Parasympathetic nerves splow down heart rate by releasing a neurotransmitter (acetylcholine) to decrease the rate of myocardial contraction
- Additionally, the heart rate may be increased by the chemical release of the hormone adrenaline into the blood (from the adrenal gland)
H.5.4 Outline atherosclerosis and the cause of coronary thrombosis
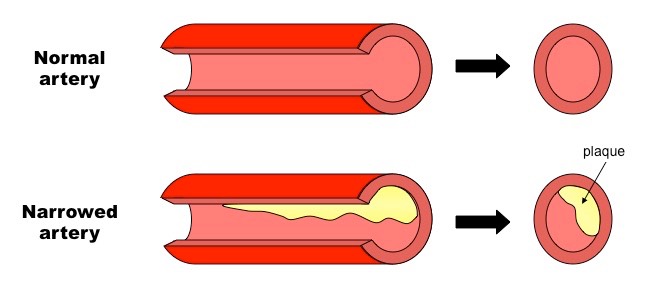
Atherosclerosis is the hardening and narrowing of the arteries, due to the deposition of material commonly known as plaque
- Damage to the artery walls (e.g. due to high blood pressure) causes chronic inflammation, leading to the accumulation of lipids, cholesterol, cell debris and calcium
- Atheromas (fatty deposits) develop in the arteries and significantly reduce the diameter of the lumen (stenosis) and reduces the elasticity of the artery wall needed for pulse flow
- This may lead to the formation of clots and blockages in the artery, and if this occurs in the coronary arteries (coronary thrombosis), it may lead to a heart attack (acute myocardial infarction)
H.5.5 Discuss factors that affect the incidence of coronary heart disease
Risk factors for coronary heart disease (CHD) include:
- Exercise – sedentary life style or excessive exercise can both place a strain on normal heart activity
- Genetics – having hypertension (high blood pressure) or a family history of heart attacks increases the risk
- Gender – males are more at risk than females due to low estrogen levels (risk increases in women post-menopause as levels fall)
- Smoking – smoking raises blood pressure because nicotine causes vasoconstriction
- Obesity – being overweight places additional strain on the heart
- Diet – too much saturated fats and cholesterol promotes atherosclerosis, high salt levels and excessive alcohol intake are also risk factors
- Age – old age leads to less flexible blood vessels